


 Sign Out
Sign Out
Absorption: Ciprofloxacin is rapidly and well absorbed from the gastrointestinal tract following oral administration. Its absolute bioavailability is approximately 70% with no substantial loss by first pass metabolism. Ciprofloxacin's maximum serum concentrations and area under the curve are shown as follows: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMaximum serum concentrations are attained 1 to 2 hours after oral dosing. Mean concentrations 12 hours after dosing with 250, 500, or 750 mg are 0.1, 0.2, and 0.4 μg/mL, respectively. Serum elimination half-life in subjects with normal renal function is approximately 4 hours. Serum concentrations increase proportionately with doses up to 1000 mg.
A 250 mg Ciprofloxacin oral dose given every 12 hours produces an AUC equivalent to that produced by an infusion of 200 mg Ciprofloxacin given every 12 hours. A 500 mg oral dose given every 12 hours produces an AUC equivalent to that produced by an IV infusion of 400 mg Ciprofloxacin given over 60 minutes every 12 hours. A 750 mg oral dose given every 12 hours produces an AUC at steady-state equivalent to that produced by an IV infusion of 400 mg given over 60 minutes every 8 hours. A 750 mg oral dose results in a Cmax similar to that observed with a 400 mg I.V. dose.
Distribution: Ciprofloxacin binds to serum proteins at 20-40%. Following oral administration, Ciprofloxacin diffuses readily into most body tissues and fluids. Ciprofloxacin is present in active form in the saliva, nasal and bronchial secretions, mucosa of the sinuses, sputum, skin blister fluid, lymph, peritoneal fluid, bile and prostatic secretions. Ciprofloxacin is also detected in lung, skin, fat, muscle, cartilage and bone. It diffuses into the cerebrospinal fluid (CSF); however, CSF concentrations are generally less than 10% of peak serum concentrations. Low levels of the drug have been detected in the aqueous and vitreous humors of the eye.
Metabolism: Four metabolites have been identified in human urine which account for approximately 15% of an oral dose. These metabolites have antimicrobial activity, but are less active than unchanged Ciprofloxacin.
Excretion: Ciprofloxacin is eliminated primarily by renal excretion. However, it is also metabolized and partially cleared through the biliary system of the liver and through the intestine.
Ciprofloxacin's serum elimination half-life in subjects with normal renal function is approximately 4 hours. Approximately 40 to 50% of an orally administered dose is excreted in the urine as unchanged drug. After a Ciprofloxacin 250 mg oral dose, urine concentrations exceed 200 μg/mL during the first two hours and are approximately 30 μg/mL at 8 to 12 hours after dosing. Ciprofloxacin's urinary excretion is virtually complete within 24 hours after dosing. Renal clearance is approximately 300 mL/minute and exceeds the normal glomerular filtration rate of 120 mL/minute. Thus, active tubular secretion plays a significant role in its elimination. Co-administration of probenecid with ciprofloxacin results in about a 50% reduction in the ciprofloxacin renal clearance and a 50% increase in its concentration in the systemic circulation. Although bile concentrations of ciprofloxacin are several fold higher than serum concentrations after oral dosing, only a small amount of the dose administered is recovered from the bile as unchanged drug. An additional 1 to 2% of the dose is recovered from the bile in the form of metabolites. Approximately 20 to 35% of an oral dose is recovered from the feces within 5 days after dosing. This may arise from either biliary clearance or transintestinal elimination.
Antimicrobial Spectrum of Activity: Ciprofloxacin is active in vitro activity against a wide range of Gram-positive and Gram-negative microorganisms.
Ciprofloxacin has been shown to be active against most strains of the following microorganisms, both in vitro and in clinical infections: See Table 2.
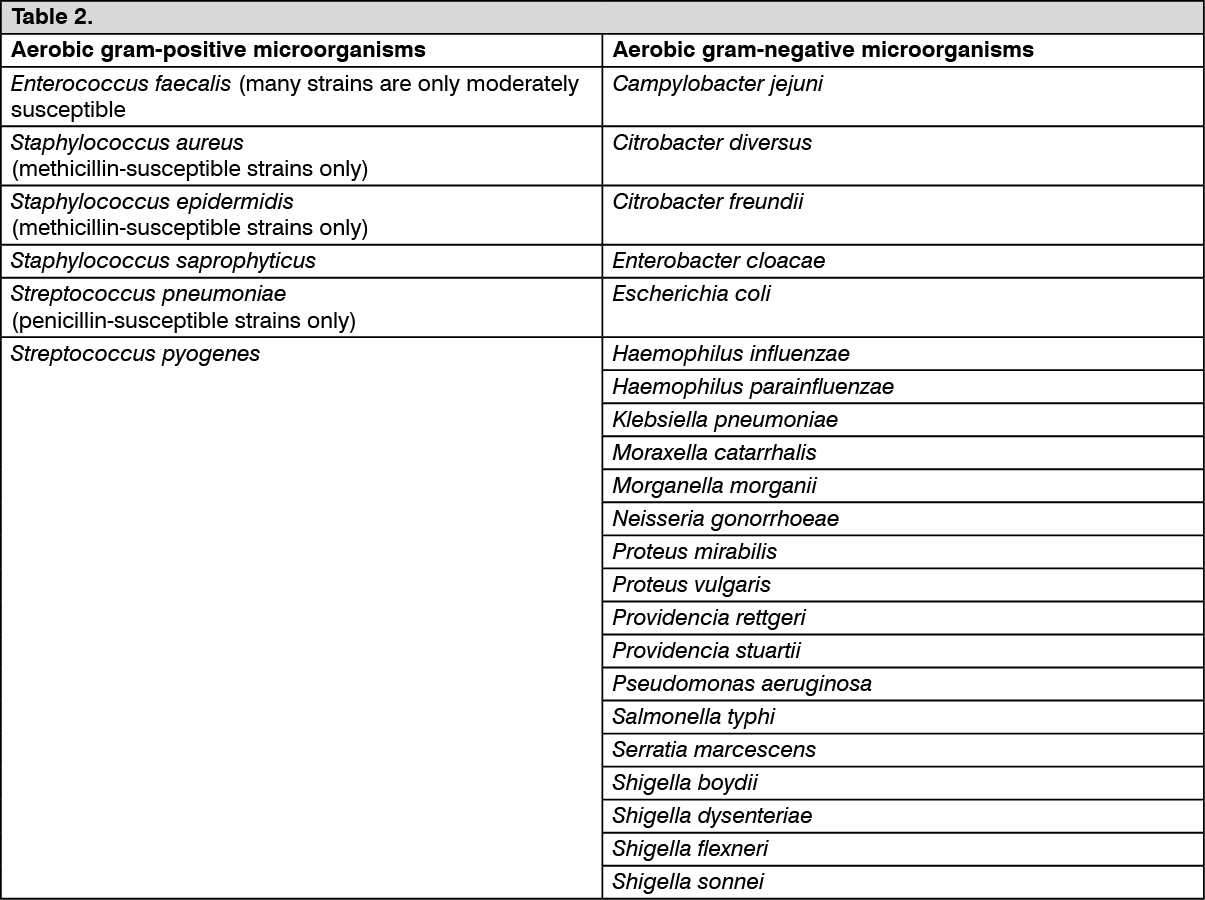 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe following in vitro data are available, but their clinical significance is unknown. (See Table 3.)
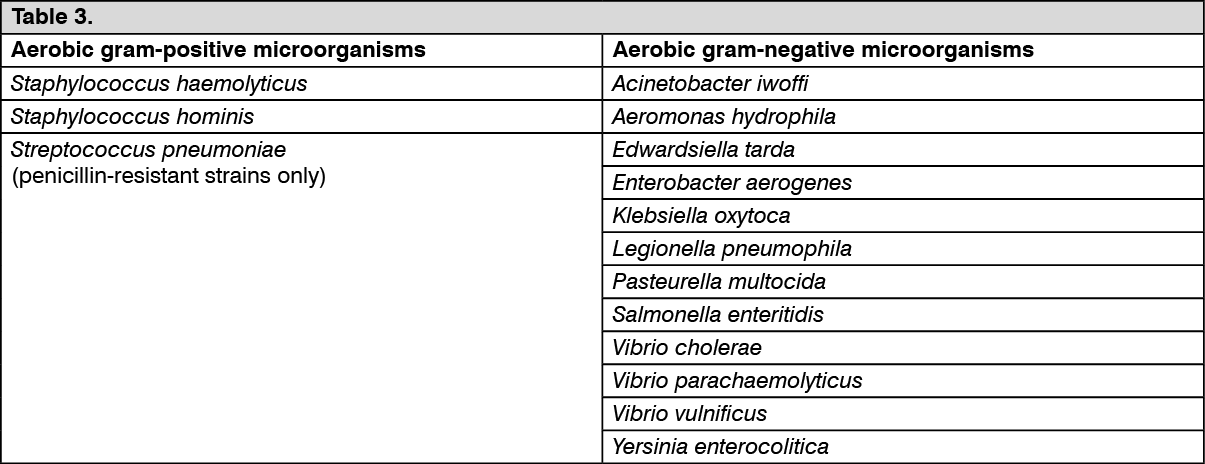 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageCiprofloxacin has been shown to be active against Bacillus anthracis both in vitro and by use of serum levels as a surrogate marker. Most strains of Burkholderia cepacia and some strains of Stenotrophomonas maltophilia are resistant to ciprofloxacin as are most anaerobic bacteria, including Bacteroides fragilis and Clostridium difficile.